--- Preventable Heart Attack Risk Factors
BEFORE: The conventional wisdom among cardiologists and most doctors is that about HALF of the risk of a heart attack can be prevented.
TODAY: The latest study presented in Munich two days ago, indicated that about 90 percent of the causes of heart attacks can be averted.
Dr.Salim Yusuf, who led the INTERHEART study that looked at cardiovascular risks in more than 29,000 people in 52 countries, presented the results last August 29th at the European Society of Cardiology Conference in Munich, Germany.
Among the risk factors identified to cause almost ALL heart attacks worldwide are:
- Smoking
- Abnormal Cholesterol
- Diabetes
- High Blood Pressure
- Stress
- Abdominal Obesity
- Sedentary Lifestyle
- Eating too few fruits and vegetables [Reuters]
According to Dr. Yusuf, "The impact of these risk factors in developing heart disease is global; it is there in every ethnic group, in men, in women, in every region of the world, in young and old. Since these risk factors may all be modified, this is remarkable and will change the way we look at heart attack prevention. It means we should be able to prevent the majority of premature heart attacks in the world."
That I think is the key word: PREVENTABLE
It means our outcome as a heart attack victim is based largely on HOW WE CONDUCT OUR LIVES. If we decide to design our lives trying to prevent or minimize most of the risk factors mentioned, even with a genetic predisposition, I think we have a fighting chance.
And while you're at it, why not grab some dark chocolate?
Another recent study says that eating dark chocolate helps prevent hardening of the arteries that leads to heart attacks. [Scotsman.com]
Dark chocos are a favorite of mine. This is great!
A word of caution though --- take it moderately, ok?
The dark chocolate study results while beneficial, "does not mean chocolate binges will ward off a heart attack." Any weight gained from eating a lot of dark chocolates would probably cancel out the apparent benefit.
Live healthy guys. You'll find it rewarding later on.
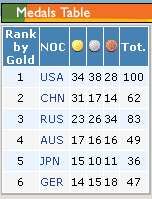 Here is the current medal tally from the
Here is the current medal tally from the 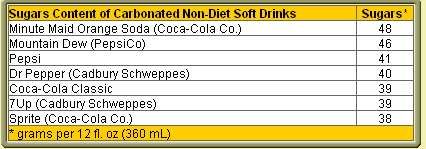 tells us that "1 of every 4 beverages consumed in America today is a soft-drink," and that picture I think is not so dissimilar here in the Philippines. In a typical meal, isn't softdrinks one of the usual orders for beverage drink?
tells us that "1 of every 4 beverages consumed in America today is a soft-drink," and that picture I think is not so dissimilar here in the Philippines. In a typical meal, isn't softdrinks one of the usual orders for beverage drink?
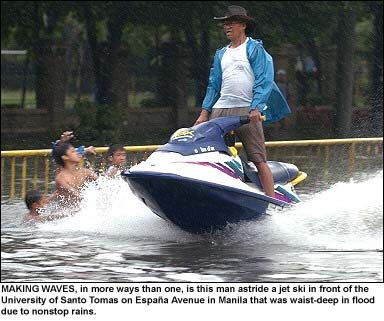 Have you been to España River? It is a couple of blocks away from my place.
Have you been to España River? It is a couple of blocks away from my place.
 "SORE EYES DOWNS WORLD'S 9th MOST POWERFUL WOMAN" was the title of the
"SORE EYES DOWNS WORLD'S 9th MOST POWERFUL WOMAN" was the title of the